Abstract
Despite over a century of advancement in social work, a critical population remains largely unexamined: individuals aging in long-term recovery from substance use disorders (SUD). This article introduces Aging in Recovery as an emerging field of inquiry and practice, situated at the intersection of recovery, aging, and social policy. Foundational contributions from Dorothea Dix, Jane Addams, Charles Loring Brace, Mary Richmond, and Saul Alinsky shaped institutional care, community practice, prevention, diagnosis, and organizing. However, these frameworks rely on visibility. This article argues that individuals aging in long-term recovery constitute a structurally invisible cohort and introduces the Aging in Recovery Residential Model (ARRM) as a practice framework within this emerging field to guide the development of recovery-informed residential and community-based environments.
Introduction: When Success Becomes Invisible
The field of social work has historically evolved in response to visible human suffering, including poverty, mental illness, child neglect, and addiction. Systems were designed to identify crisis, intervene, and stabilize. Yet recovery introduces a paradox. Individuals who sustain 15, 20, or 30 years of recovery often achieve what systems were designed to produce: stable employment, family reunification, economic security, and community integration. They become, by all observable measures, successful.
Beneath that stability, however, remains a critical reality: recovery is not the absence of damage, but the ongoing management of it. The physical, neurological, psychological, emotional, and spiritual consequences of substance use persist across the lifespan. Individuals in long-term recovery may continue to manage chronic health conditions, trauma histories, emotional regulation challenges, identity reconstruction, and vulnerability to relapse (Kelly et al., 2017; Kuerbis et al., 2014). Once stability is achieved, formal systems often disengage. In this way, recovery success can produce structural invisibility.
A Profession Built on Visibility
The foundations of social work reflect a consistent pattern: responding to visible need. Dorothea Dix exposed institutional suffering and called for public responsibility. Jane Addams embedded services in neighborhoods, making social conditions visible through proximity. Charles Loring Brace identified neglected children as a social concern requiring organized intervention. Mary Richmond formalized assessment and case-based intervention. Saul Alinsky demonstrated that power emerges from organized, visible constituencies (Alinsky, 1971; Richmond, 1917).
Across these traditions, one principle remains clear: systems respond to what they can see. But what happens when success reduces visibility?
From “Dangerous Classes” to Criminalization
In The Dangerous Classes of New York (1872), Brace framed marginalized populations as both vulnerable and socially threatening. That dual framing echoes through later punitive approaches to addiction. Twentieth-century drug policy, including the Rockefeller drug laws and the War on Drugs, focused on active addiction as a problem of crime, pathology, or crisis. These systems were built to respond through punishment, treatment, or emergency intervention, not to sustain recovery across decades.
Treatment Systems and Their Limits
Modern treatment models, including therapeutic communities, were shaped by institutional and diagnostic traditions that emphasized stabilization, behavioral change, and early recovery. These approaches play an important role, but they are not designed to address the long-term recovery trajectory across the lifespan. They are built to help people enter recovery, not to support them as they age within it.
Mutual Aid: The Unrecognized Continuum of Care
The community-based logic of Addams and the organizing logic of Alinsky are reflected in mutual aid movements such as Alcoholics Anonymous and Narcotics Anonymous. These systems provide what formal systems often do not: continuity, belonging, identity, and lifelong support. Yet because they are decentralized, voluntary, and often anonymous, they remain largely invisible within formal policy, research, and service systems.
The Invisible Cohort: A Growing Demographic Reality
Empirical research confirms that recovery is both real and sustained. National survey data suggest that millions of Americans identify as being in recovery (Substance Abuse and Mental Health Services Administration [SAMHSA], 2020). Sustained remission over time is associated with a significantly reduced risk of relapse and improved functioning (Kelly et al., 2017). At the same time, older adults with substance use histories experience elevated rates of chronic illness, cognitive impairment, and age-related vulnerability (Han et al., 2020; Kuerbis et al., 2014). Aging populations also face increased risks of isolation and depression (Blazer & Wu, 2009).
Despite these findings, minimal research has focused specifically on individuals aging in long-term recovery. They no longer fit within treatment systems, are often outside formal mental health care, and are rarely recognized within aging services. They are not absent. They are unseen
Aging in Recovery as a Field
Aging in Recovery represents an emerging field that examines recovery as a lifespan process shaped by biological aging, long-term health outcomes, identity, structural invisibility, and changing social roles. Yet unlike more established domains in social work, this field lacks dedicated service systems, standardized assessments, longitudinal research, and clear policy recognition.
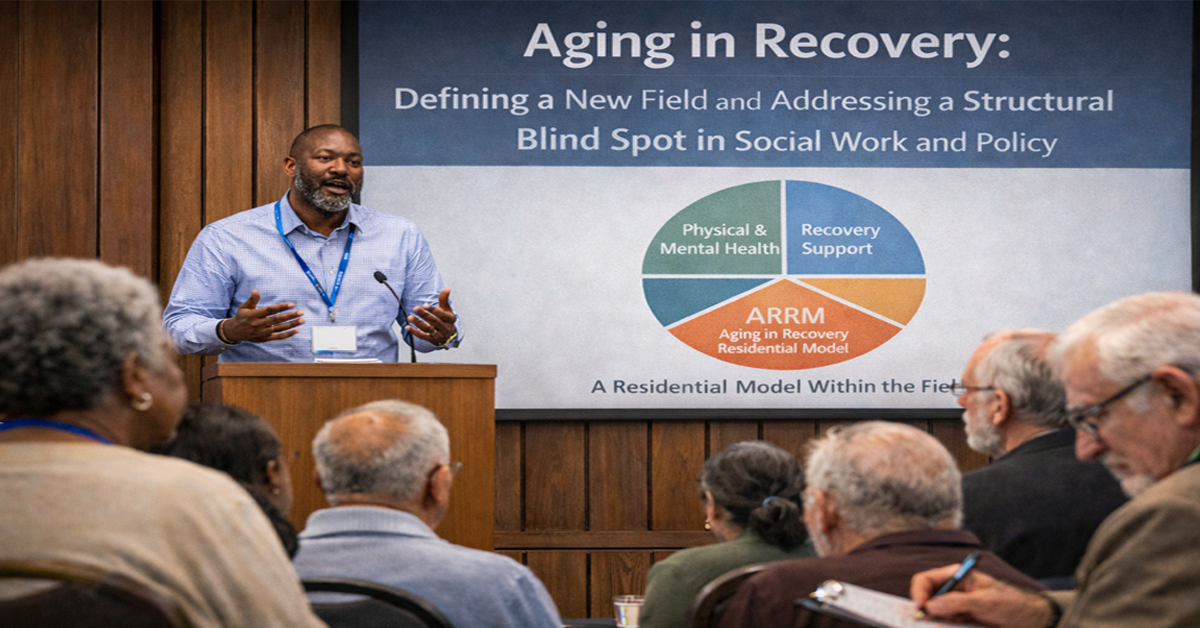
ARRM: A Residential Model Within the Field
The Aging in Recovery Residential Model (ARRM) is proposed as one structural framework within this emerging field. ARRM is not a general response model or an abstract conceptual category. It is a residential and environmental model intended to guide the design of recovery-informed living environments and community-based residential settings for individuals in long-term recovery entering later life.
Its core principle is straightforward: systems are designed to initiate recovery, but not to sustain individuals in recovery as they age.
ARRM shifts the focus from episodic intervention to continuity of environment. It recognizes that long-term recovery is sustained not only through treatment or personal determination, but through settings that reinforce dignity, peer connection, purpose, stability, and non-clinical supports over time. In this framework, residential environments are not passive backdrops. They are active components of long-term recovery maintenance.
Like earlier social work innovations that linked environment and well-being, ARRM offers a model for organizing supportive residential and community life around an emerging social condition: aging in long-term recovery.
The Central Question: What Are the Needs?
The absence of infrastructure in this field reflects a failure to ask the question, not a lack of need. Emerging domains include health and aging, mental and emotional continuity, social connection, recovery sustainability, and the diverse ways race, class, gender, and recovery pathway shape later-life experience. Individuals aging in recovery are not a monolith, and ARRM requires an intersectional, individualized approach.
Implications for Social Work
Aging in Recovery represents an important next step in the evolution of social work. It calls for a shift from crisis to continuity, from intervention to lifespan support, and from invisibility to recognition. Social work must expand beyond early recovery and acute care to engage long-term recovery as a legitimate practice and policy concern.
Conclusion
The foundations of social work were built on making suffering visible. But recovery has produced a population that no longer fits neatly within those traditional frameworks. Individuals aging in recovery are not absent. They are unseen.
Aging in Recovery is an emerging field that reflects a present and growing reality. The Aging in Recovery Residential Model offers one framework for beginning to address that reality through continuity-based, recovery-informed living environments and long-term support structures. The question is no longer whether this population exists. The question is whether we are prepared to recognize it and build accordingly.
References
Alinsky, S. D. (1971). Rules for radicals. Random House.
Blazer, D. G., & Wu, L.-T. (2009). The epidemiology of substance use disorders among older adults. American Journal of Psychiatry, 166(10), 1162–1169.
Brace, C. L. (1872). The dangerous classes of New York and twenty years’ work among them. Wynkoop & Hallenbeck.
Han, B. H., Moore, A. A., Sherman, S., Keyes, K. M., & Palamar, J. J. (2020). Demographic trends of binge alcohol use and alcohol use disorder among older adults in the United States, 2005–2014. Drug and Alcohol Dependence, 170, 198–207.
[Note: if you used a different Han et al. source, swap this for the exact citation.]
Kelly, J. F., Greene, M. C., & Bergman, B. G. (2017). Recovery from substance use disorder: A systematic review of definitions, prevalence, and correlates. Drug and Alcohol Dependence, 181, 162–169.
Kuerbis, A., Sacco, P., Blazer, D. G., & Moore, A. A. (2014). Substance abuse among older adults. Clinics in Geriatric Medicine, 30(3), 629–654.
Richmond, M. E. (1917). Social diagnosis. Russell Sage Foundation.
Substance Abuse and Mental Health Services Administration. (2020). National survey on drug use and health. U.S. Department of Health and Human Services.
White, W. L. (2007). Addiction recovery: Its definition and conceptual boundaries. Journal of Substance Abuse Treatment.